
Emily Smith's Blog
April 13, 2026
Neighbor Monday: War and children
Children are always disproportionately affected by war. An estimated 1 in 5 children globally live in conflict zones. And, the number of attacks on health facilities is increasing. So, if children get hurt due to war (or during a war just because they are kids and get hurt or sick at times), the ability to take care of them (and their families) is impacted if the doctors and hospitals are gone.
The British Medical Journal reported that the number of attacks on healthcare facilities has tripled since 2020. The graph below shows the main areas where conflict has occurred
Friendly Neighbor Epidemiologist is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
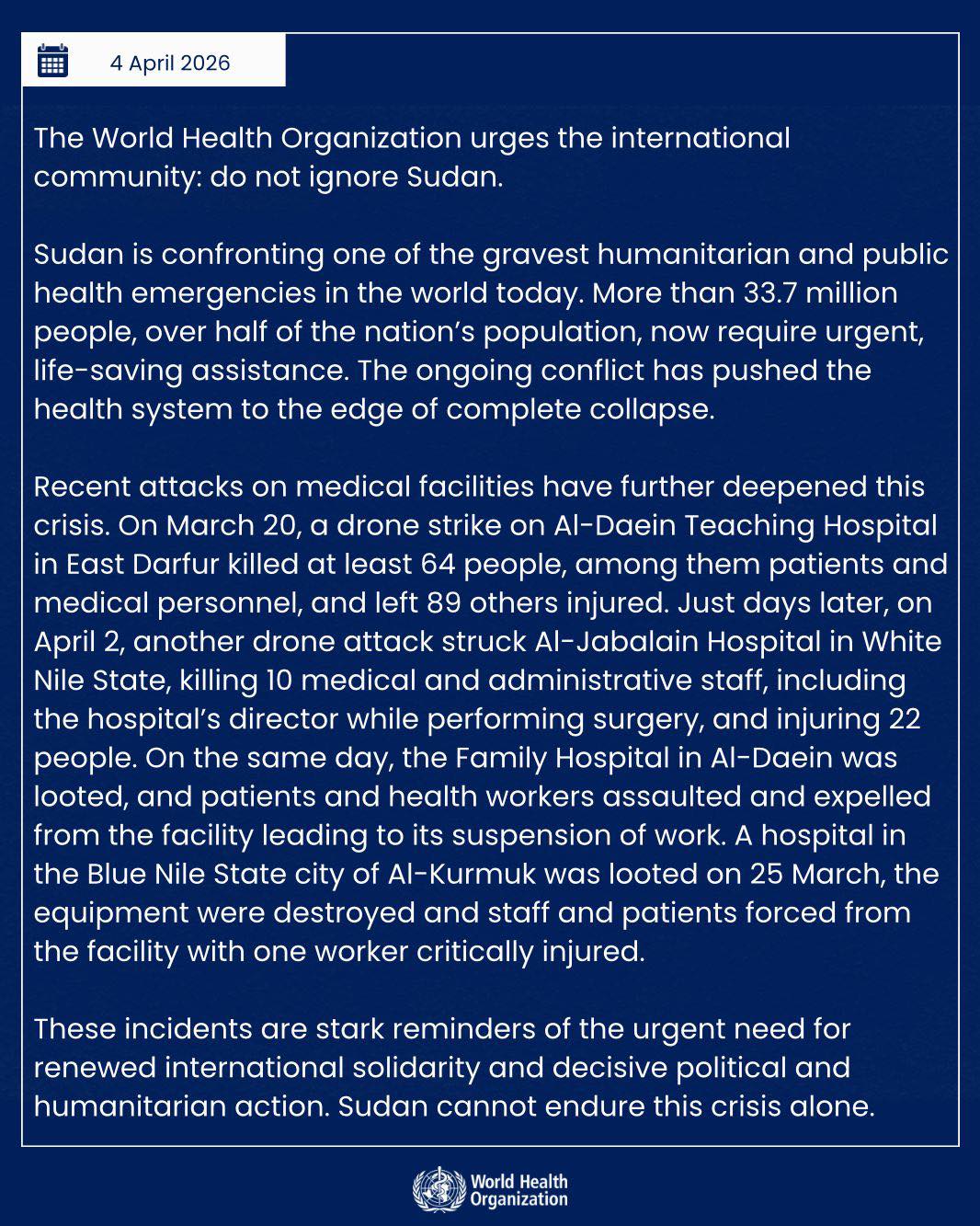
For example, in Sudan, there have been 649 attacks on healthcare facilities from 2020-2024. Since 2023, 70-80% of facilities in Sudan are completely destroyed or non-functional.
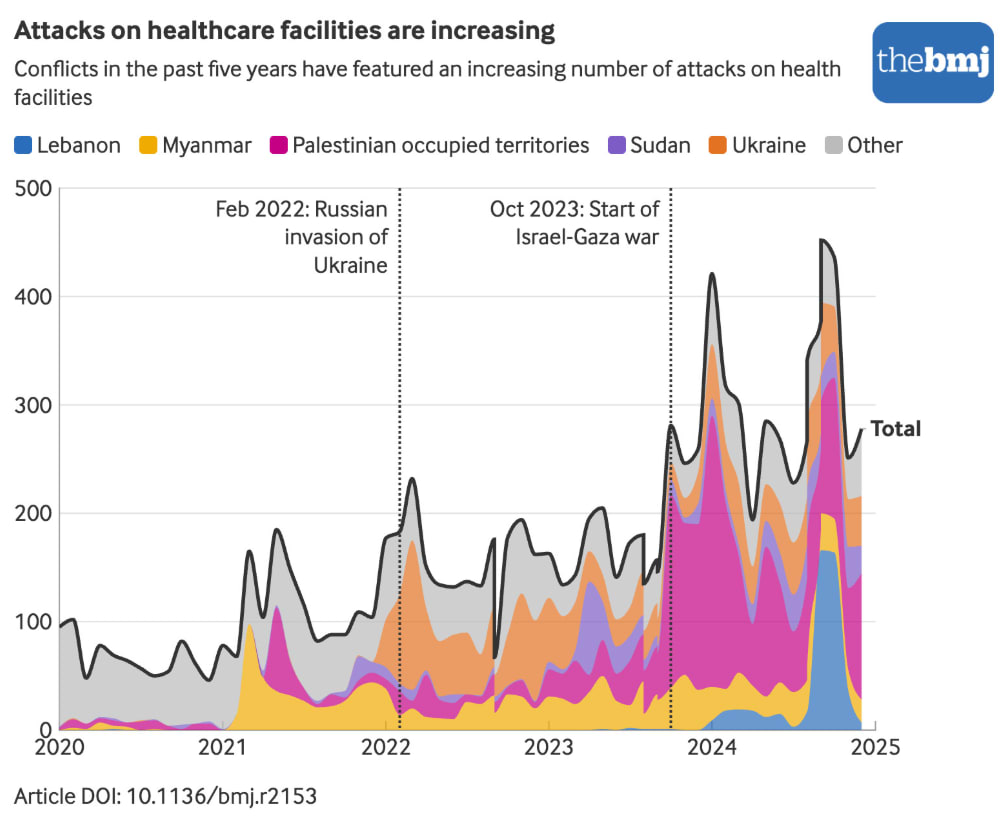
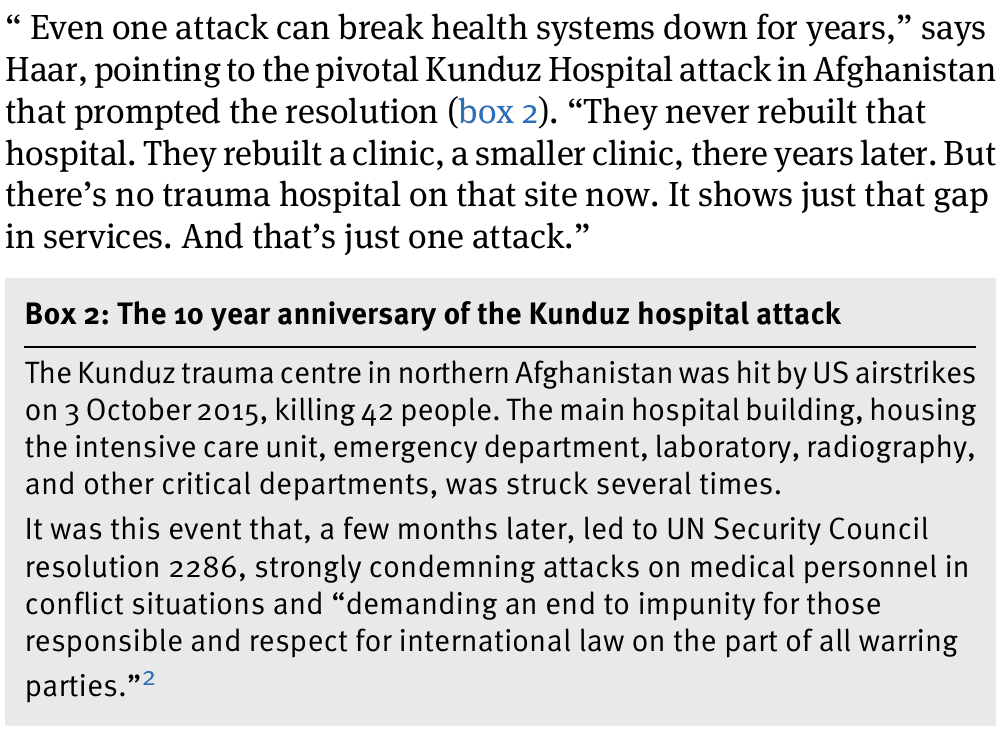
In fact, the BMJ article I referenced above is titled “How attacking healthcare has become a strategy of war”. It’s not just about the war (although that in and of itself is enough for us to care as neighbors). It’s now about dismantling health systems that will last for years. Here’s an excerpt from the article:
In my own work, I’ve partnered with St. Jude to estimate the impact of war on children’s cancer care. In my day job, my main research projects are centered on the intersection of poverty and children’s health. And, since most armed conflict/war happens in areas with high poverty, the impact of that war is directly on the children I encounter (and their families).
400,000 children are diagnosed with cancer every year, and a whopping 90% of those children live in low-income countries. The mortality disparity for children with cancer is one of the highest in global health - the same percentage of children surviving cancer in the US and other high-income countries are dying from cancer in low-income countries. It’s almost a direct 80/20 split.
80% of children survive cancer in high-income countries.
80% of children die from cancer in low-income countries.
And the problem isn’t really an issue of biology or the cancers in low-income countries being harder to treat. The issue is systemic and structural. The diagnostic needs (think biopsises, CT scans, MRIs etc) and treatment capabilities (think chemo and radiation) are not available in most low-income countries (unless you live in a capital city and can afford that care). Most children with cancer live in rural areas and the families simply cannot pay for the transportation or lodging to get to the capital city for a diagnosis, let alone the treatment costs.
Then war hits. Healthcare facilities are decimated. Healthcare workers are injured or killed. What do the children with cancer do?
For some children, St. Jude (and other great organizations) can swoop in to take the child and their families to the US or Germany or somewhere to remain in their cancer treatments. For many of these children, remaining in that care is a matter of life or death. If you stop treatment, you can’t take a few months off and then resume after the war subsides. Any treatment abandonment or pause can be catastrophic to a child with cancer because the tumor can begin growing and spreading again.
When Ukraine was attacked by Russia, St. Jude worked quickly with their in-country partners to help the kids receiving treatment or in need of cancer treatment through SAFER Ukraine. They have helped over 1,400 Ukrainian children evacuate to continue treatment in the US, Canada, or Europe.
SAFER Ukraine created a registry to keep track of children whose medical records have been translated, and who have been evacuated or whose cases are being monitored. The registry currently includes more than 1,100 Ukrainian patients.
The main people in charge of this program are my colleagues, Dr. Paul Wise and Dr. Asya Agulnik, and they are some of the best neighbors I know.
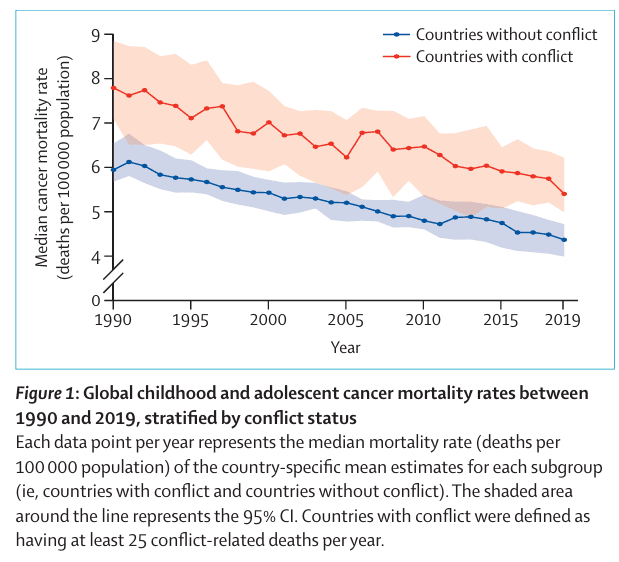
We wanted to look at the impact of war and children’s cancer from a global perspective. So, we set out to do just that, and it was published in Lancet Oncology. We looked at the impact of war and armed conflict on children’s mortality rates over the past few decades, and here’s what we found:
Over time, cancer mortality rates for children have decreased. But it depends on where you live. In countries with conflict (red line), the rates have stayed frustratingly high.
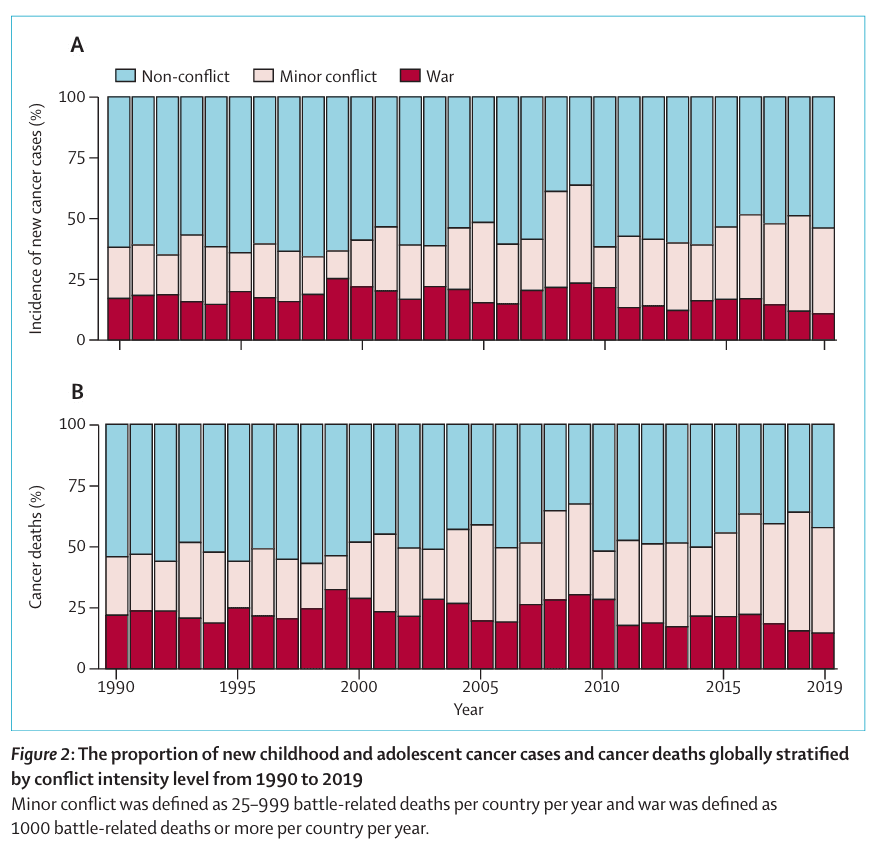
The biggest take-away for me is that the number of children dying from cancer is growing the most in countries with minor levels of conflict. These are countries that don’t have a full war (defined as over 1,000 battle-related deaths), but have lower levels of chronic conflict. To me, that means that even lower levels of war can greatly impact instability in the country, disrupt health systems (many of which are already barely hanging on), and trickle down to impact children’s ability to get to cancer care when they need it.
 FINAL THOUGHTS
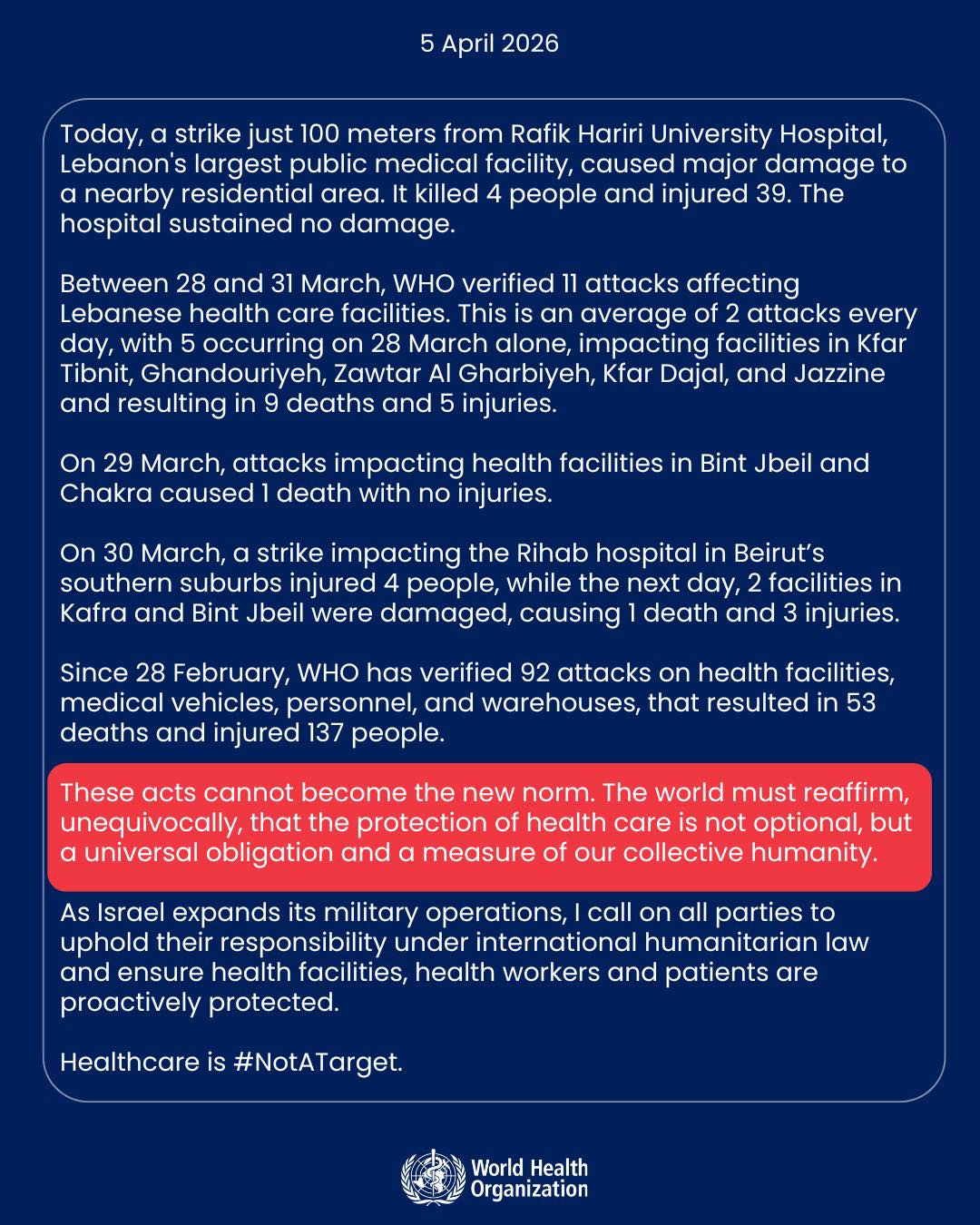
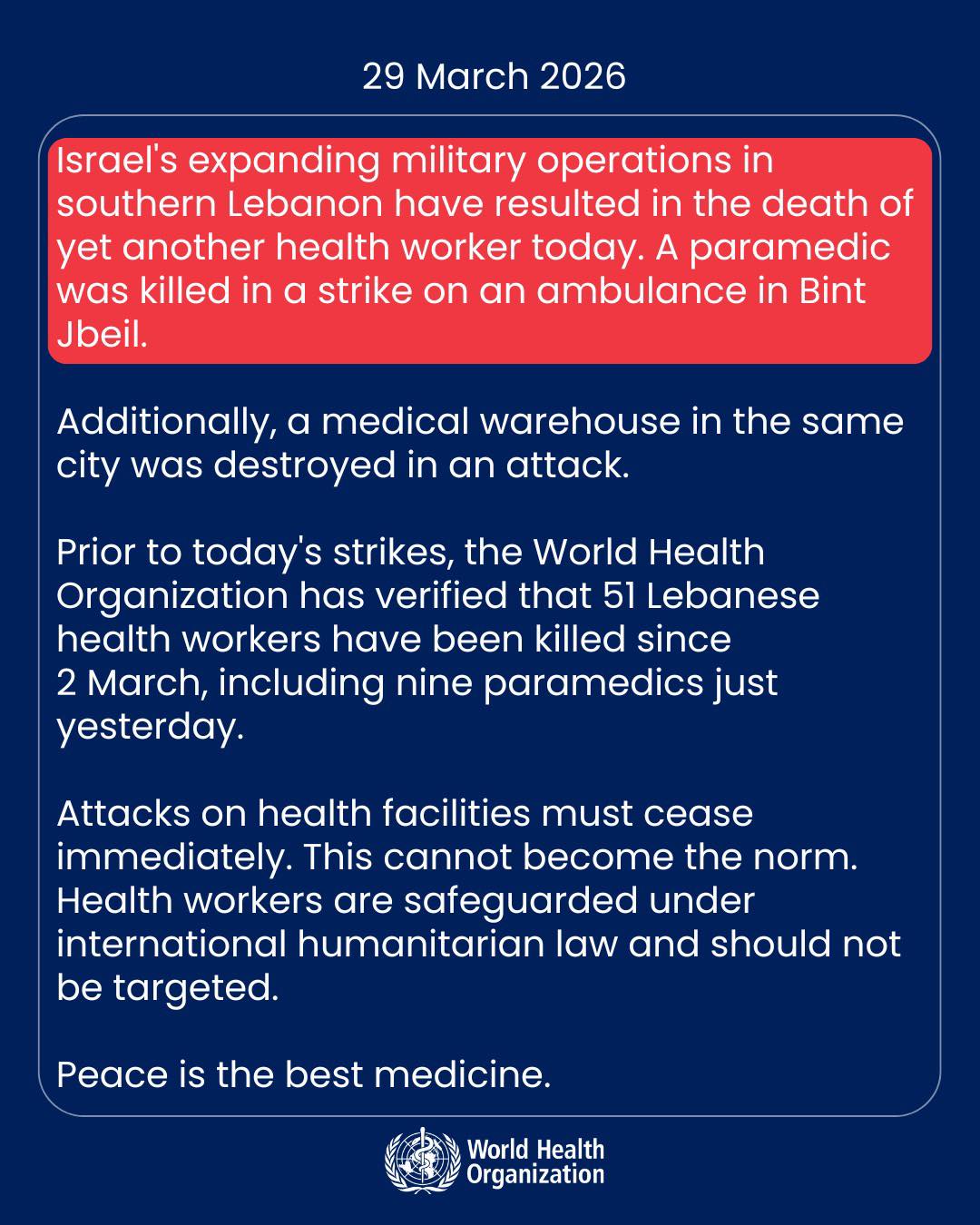
FINAL THOUGHTSIn an ever-changing world with war now in the Middle East, I’m thinking of the direct impacts of war that make the news. And, also. I’m thinking of the families caught in the crosshairs of a conflict not of their making. I showed you the data of my own work for children with cancer, but this could easily be a proxy for children with malaria. Or mothers who need their prenatal care. or Grandfathers with tuberculosis or diabetes or COVID who need medicine. War is never fair, especially to those with health needs. I want to end this with a powerful quote from Dr. Wise that steadies me when I’m doing my own research. And some recent quotes from Dr. Tedros Adhanom Ghebreyesus, Director General of the WHO, about the impact of the current war in the Middle East on health.
Let it be an encouragement to us all to keep neighboring in the hard places.
-Emily
PS: After these types of posts, I always get emails about how to help support this work. If you want to contribute to my work with children with cancer, you can donate at this donation link. We set up a fund through Duke so all donations are tax-deductible.
Thank you so much to those who have donated over this past year! It has helped keep my US-based and Africa-based team afloat for one more year! If you’re curious about where the donations go, here’s a quick breakdown of my work and team.
For other ways to donate via check or QCD:
If sending a check, please make the check payable to Duke University, but include “Emily Smith - Global Children’s Cancer Fund - 391001207” on the memo line or in an included note. You can send the check to:
Duke Children’s Development (Duke Children’s Hospital)
300 W. Morgan Street, Suite 1000
Durham, NC 27701
If donating via QCD, Duke’s tax EIN is 56-0532129.
For any questions, you can email globalhealth.giving@duke.edu and emily.smith1@duke.edu and we can help get your donation to the right place.
Friendly Neighbor Epidemiologist is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.


March 28, 2026
Be relentlessly intentional towards joy
 Photo by James Wainscoat on Unsplash
Photo by James Wainscoat on UnsplashDid I ever tell you about the time I found a love for hummingbirds? When I was growing up, my West Texas grandparents would take us camping to Cloudcroft, New Mexico. Those were the ‘big mountains’ to those of us who grew up in the desert or flat-plains of Texas/New Mexico. (It would be years later before I went to Colorado and had to redefine what ‘big mountains’ meant. Ha!) But, Cloudcroft was magical to us grandkids. We explored and wandered and imagined. My Granddaddy always found the perfect spot to park the camper that seemed extra magical. Then, my Grandmother would hang the hummingbird feeders. And, that’s where I learned to put your finger on the landing spot, stand really still, and wait. And, wait some more. Because at some point, the hummingbirds would come over. AND LAND ON YOUR FREAKIN’ FINGER. Guys, this was delight upon delight to my 10-year-old-self.
I’ve thought a lot lately about this type of delight. Mainly because I’ve told my husband more times than I can count this week that I’m determined this time around to not let stress or despair or the awfulness of the world win. During 2020-2021, the awfulness plowed me over eventually and knocked me down for months at a time. It (‘it’ being threats at the house, against my kids, losing a church, friends, community, moving, more threats) was too much, and my body, who had been keeping the score, would protest with a strong ‘no more!’, landing me fully in bed for ~18 months.
March 21, 2026
"Peace" through War, the National Prayer Breakfast, and Iranian schoolchildren being killed
 A funeral ceremony for students and staff members of Shajareh Tayyebeh elementary school on March 3. (Ircs / ZUMA Press Wire via Reuters Connect)
A funeral ceremony for students and staff members of Shajareh Tayyebeh elementary school on March 3. (Ircs / ZUMA Press Wire via Reuters Connect)“The prophet Jeremiah spoke against prophets who were proclaiming “peace, peace, when there is no peace”.
I keep thinking back to a few weeks ago when I was at the National Prayer Breakfast. I’ve had the hardest time figuring out how to write this post ever since Israel and the US bombed Iran. Remember me telling you that I walked out of the National Prayer Breakfast in DC when Pete Hegseth said that “peace” comes through violence/war because that’s what the Bible said? (ugh!) In my reflection post about the Prayer Breakfast, I mentioned the room felt unsafe - well, it felt worse than that. It felt violent. It was a call to a war and violence in the name of religion. And, violence was discussed over and over again. It was weird and scary and definitely not Jesus.
Fast forward a few weeks to when Iran was bombed. I instantly remembered the remarks about violence from Trump, Hegseth, and others.
March 19, 2026
A Lent prayer from me
 Photo by Zach Lezniewicz on Unsplash
Photo by Zach Lezniewicz on UnsplashO Lord, you gave us an example of what a neighboring table should look like.
One of humility and of love. Of giving out our lives in the service of others rather than grasping for power over others.
You showed us that you can multiply our meager portions of a few loaves and fish to feed a multitude of people. Our ‘this is all I have right now’ turns into abundance through you. It’s enough.
At your table, you declare blessings over the poor, the destitute, the hungry for justice, and the thirsty for righteousness.
You preached about freeing the captives, you stopped entire crowds for a bleeding woman who spent everything she had on healthcare, you centered the child in your midst, you stopped a teaching to let a sick man be lowered from the roof, you spoke with a woman who just wanted to remain hidden at a well, you made sure your mom was taken care of before you died, you touched the untouchable and loved the unlovable, you ate with the ‘wrong’ crowd, blessed the ‘wrong crowd’, and washed the feet of the ‘wrong’ crowd.
O Lord, this way of neighboring seems so upside down to me.
But, perhaps that’s the point. Perhaps the point of you flipping the script shows us how to live out our faith in these days. A faith of being assured of things not seen yet but promised. A life of living the here-and-not-yet but hoped for.
I want to do the same.
And, sometimes that takes flipping tables over that I’m sitting at.
Lord, during this Lent season, let us remember the upside-down way of faith. Let us flip over tables that we are not meant to sit at and sit at the ones you are at.
Your tables are the tables of enoughness for all rather than a select few.
They are the tables you set in the middle of war zones and enemies.
They are the tables you break bread at, pointing us towards a new way of life, and reminding us to give thanks.
They are the tables where you bring the poor to the head of the table and the least are given the seats of honor.
Those tables, O Lord, those tables are ones of abundance and justice and equity.
Help us see the tables we are seated at that need to be flipped over and left. And find the ones you have prepared for us.
Help us during the lonely and confusing and tiring moments to find the tables of restoration, of living water, and of thanksgiving bread.
You, O Lord, prepare a table for us in the middle of the wilderness.
May we find it during this wilderness time. When we can’t, guide us with your gentle and strong shephardness. When we mourn for how things should be, remind us that that’s our hearts aching along with the Spirit.
You alone prepare the table for us.
May we sit at it and weep and feast and rest and love.
May our hearts journey in the long obedience towards your table of neighboring through faith during this Lent season.
Amen.
*Originally written in 2025.
March 10, 2026
Neighbor Tuesday: Measles update
Welp, measles continues to climb. (boo! hiss!) Measles in the US is now ~1300 cases to date - and that’s only the confirmed cases. Because measles is so contagious (every person infected with measles can infect 10-12 others), that number is likely a LOT higher.
To put this in perspective, let’s look at 2025. For ALL of 2025, there were 2,283 confirmed cases - total. Now in 2026, we are already nearly half of that, and it’s barely March. 93% of cases are among unvaccinated (or vaccine status unknown) individuals and 78% are in children/adolescents.
 Measles Cases and Outbreaks | Measles (Rubeola) | CDCWhere is measles spreading?
Measles Cases and Outbreaks | Measles (Rubeola) | CDCWhere is measles spreading?Geographically, certain states seem to be hit hard so far. I’m sure you’ve heard of the Texas and South Carolina outbreaks. But, have you heard about Utah and Florida? I hadn’t heard much about those states! It goes to show that measles can increase ‘under-the-radar’ rapidly among unvaccinated populations. In 2026, Utah has the most new measles cases of any state except South Carolina. State-level immunization coverage is below national averages and definitely below the herd immunity rates needed to control measles. Of the 358 measles cases since June 2025, only 8-10% were vaccinated. One pediatrician in Utah stressed how serious measles can be with kids being “very, very ill” with high fevers, severe coughing and pneumonia.
In Florida, the childhood vaccination rates have declined over recent years and is now 89% (under the 95% herd immunity rate). Among younger children, only 76% are fully vaccinated (a massive drop from 86% a decade ago).

Let’s compare the above map to the % vaccinated populations.
 Measles is not a “cold” and Vitamin A won’t cure it.
Measles is not a “cold” and Vitamin A won’t cure it.Measles is the most infectious disease in the world.
9 out of 10 people will become infected with measles if exposed and not protected through vaccines. Measles can survive for 2 hours in the air or on infected surfaces (like doorknobs, light switches, tables, etc) and spreads when an infected person breathes, coughs, or sneezes. An infected person can transmit measles to others from 4 days prior to the rash starts. Yikes. Here’s a map of measles cases in the US in April 2025. Compare that to the map above and you can easily see it's spreading - rapidly.

There is no specific treatment for measles. You’ve probably heard a lot about vitamin A being used to try to treat measles. That can actually backfire pretty badly, with high levels of vitamin A leading to liver damage and toxicity.
30% of children infected with measles develop a complication. Complications include blindness, brain swelling/damage, pneumonia or other breathing problems, severe diarrhea leading to dehydration, and infections. Some of those complications can happen years after infections. 1 in 5 will need hospital care.
For pregnant women, measles can be super dangerous to her and the baby and lead to miscarriage, premature birth, and stillbirth. The MMR vaccine works incredibly well to protect us, our children, and our neighbors against measles. And, measles is not a simple cold. It can lead to severe disease and even death in some cases. There’s no treatment other than supportive care. And, vitamin A won’t cut it.
The scariest part to me as a mom and epidemiologist.But, the main take-home point for me is the long-term implications of a measles infection. The scariest part for me when my kids were little was knowing that a measles infection could be mild but then show up with severe complications years later. In other words, it can lie dormant for years (average of 7-11 years) and then land your kid in the hospital with neurological damage and a high risk of death. I didn't want to chance that or the other awful outcomes a measles infection can cause in children. I also remember wanting to protect myself after my first child was born and we were trying for another baby. Measles can be so scary during pregnancy for both the mom and the child - but especially for the child with a high risk of miscarriage or stillbirth. The MMR vaccine is safe and your greatest defense for you and your family against these very real outcomes.
Does the vaccine work?The MMR vaccine works extraordinarily well. In fact, the vaccine is more effective at reducing cases and deaths than any other vaccine we currently have. I can’t emphasize this enough. The MMR vaccine is the top of the class when it comes to vaccines. Two doses of the MMR vaccine are ~97% effective at preventing measles. WHOA! That’s incredibly high protection against measles. Check out the impact on the next graph - prior to the MMR vaccine, the US had ~75,000 cases of measles each year. After the MMR came around, that dropped dramatically.
In the US, check out the graph below. Measles was pretty much eliminated in the US before making a comeback in 2019.
 caption...Measles here in NC
caption...Measles here in NCMeasles is here in North Carolina where I live. I work at one of the most premier universities and well-equipped hospital systems in the US. My hospital has some of the best physicians and facilities to help our sick neighbors. People come from all over to receive life-saving treatments for cancer, autoimmune disease, transplants, etc. And, ALL of those patients are immuno-compromised and are at a higher risk of severe disease and complications from measles. For patients with cancer or those undergoing a transplant, they have to wait months after finishing treatment to receive a MMR vaccine against measles. So, if you have a family member or friend undergoing treatment or is immunocompromised, you can help protect them against measles complications by being fully vaccinated yourself. And your kids and the rest of the family. To me, it’s just too risky to be overly cautious with measles - especially since 1 infected person can spread to 9-12 others.
A final wordI know there’s so much happening in the world right now, and the news has moved on from measles. But, remain vigilant if you’re in a state that is increasingly seeing measles infections like mine. Make sure you and your family are vaccinated. If you have a small child or a high-risk family member (like someone going through cancer treatment), consider limiting playdates or vacations with families you know aren’t fully vaccinated. I totally recognize that it can be awkward and hard! I get that on a very personal level. But take courage and do what you need to do.
Hang in there, neighbors! I put the links below for other posts I’ve done on measles if you need more information.
-Emily
Neighbor Tuesday: Measles in my hometown, flu everywhere, and RFK Jr.
MMR vaccine: Just the basics from a mom and scientist
Measles update. Should you get a booster and how to protect yourself and your family?
Vitamin A, herd immunity, the pastor in Texas, booster info, and cases are not normal this year.
March 8, 2026
Ice-dancing, self-criticism, and freedom
 Photo by Anita Austvika on Unsplash
Photo by Anita Austvika on UnsplashAnyone love the Olympics? Ever since my kids were small, I’ve loved watching the Olympics and have used those seasons to try to teach them about the wonderful world we live in - complete with Olympic cookies, a “trip around the world” in the house, and a HUGE tent in the living room. (You can see the pictures and read about that here!)
This year, like many of you, I was captivated by the ice dancing. Watching Alysa Liu bring her full self as she danced, twirled, jumped, and skated, boldly celebrate, and defy what female ice skaters “should” look like was magical.
I was also captivated by the ice dancing competition and am now watching the Netflix series on the top teams. In the documentary, one of the female competitors was talking about teaching her younger students how to not only skate on the ice but live there freely (at least, that’s how I interpreted it).
February 25, 2026
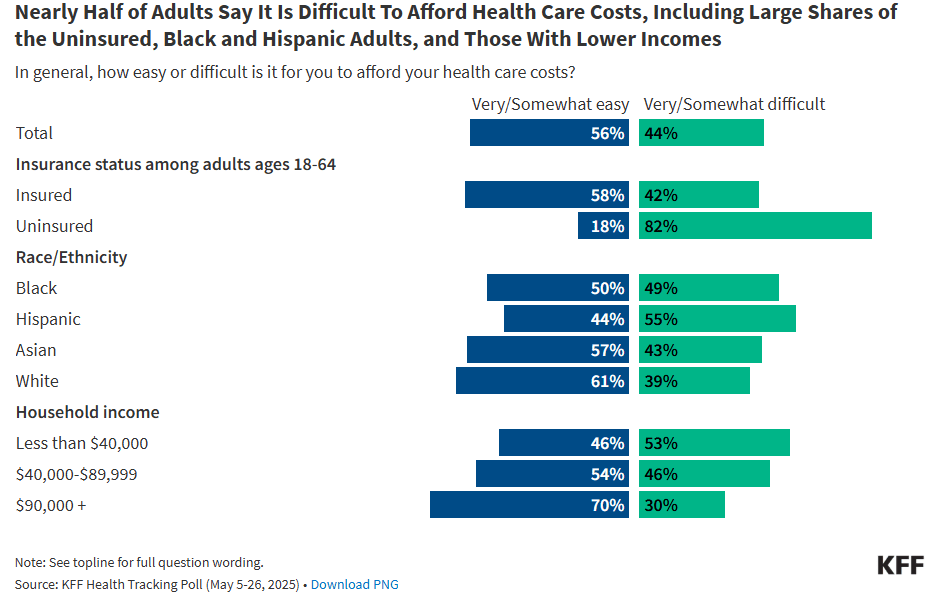
Neighbor Wednesday: Unaffordable health insurance (or losing ACA subsidies)
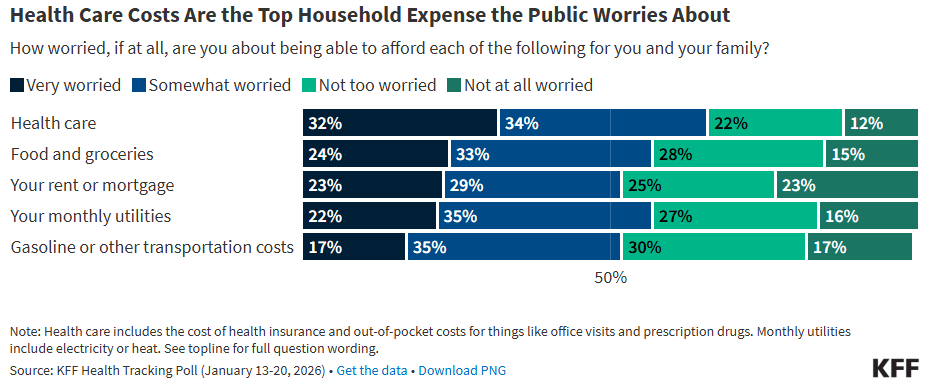
Phew, things are expensive out there, am I right? I was listening to a favorite podcast when the host mentioned housing prices increased by 40%, 50%, 60% over the past few years. Top that with a 19% increase in food, inflation, rising property taxes, and insurance rates, and we are seeing the highest monthly costs in the US since the first data was collected more than 3 decades ago.
To put it simply, families are pinched. Families who were already struggling with food insecurity and poverty are doubly (triply+++) so now.
Now that the Affordable Care Act (ACA) subsidies have expired, insurance rates have skyrocketed.
What’s the ACA?The ACA was enacted in 2010 to expand health insurance to uninsured individuals through a marketplace with varying premiums based on their incomes. And it was a big success! An analysis of how the ACA helped people access health insurance found:
“Among non-Hispanic Black individuals, marketplace enrollment among eligible individuals more than tripled, from 10.3% prior to the subsidies to 31.0% after implementation.
Among Hispanic individuals, enrollment among eligible individuals increased about three-quarters, rising from 13.3% to 23.4%.
Among rural residents, enrollment among eligible individuals more than doubled, from 12.6% to 25.6%.
Among children 18 and under, enrollment among eligible individuals nearly doubled, from 18% to 35.8%.
Among part-time workers, enrollment among eligible individuals increased by more than two-thirds, from 20.2% to 34.5%.”
“These are not incidental changes,” Jacobs [study author] says. “Before the enhanced subsidies, there were large gaps in who took up marketplace coverage across racial and ethnic groups. After the subsidies, those gaps essentially disappeared. This tells us the enhanced subsidies changed who could realistically afford insurance.”
This means that families can afford health insurance and the premiums are lower. For example, a low-income family of four would pay nearly 7% of its total monthly income for health insurance without the ACA. However, the percentage dropped to 2% with the ACA subsidies - meaning that the families had more money left in their bank account to pay for food, rent, daycare…
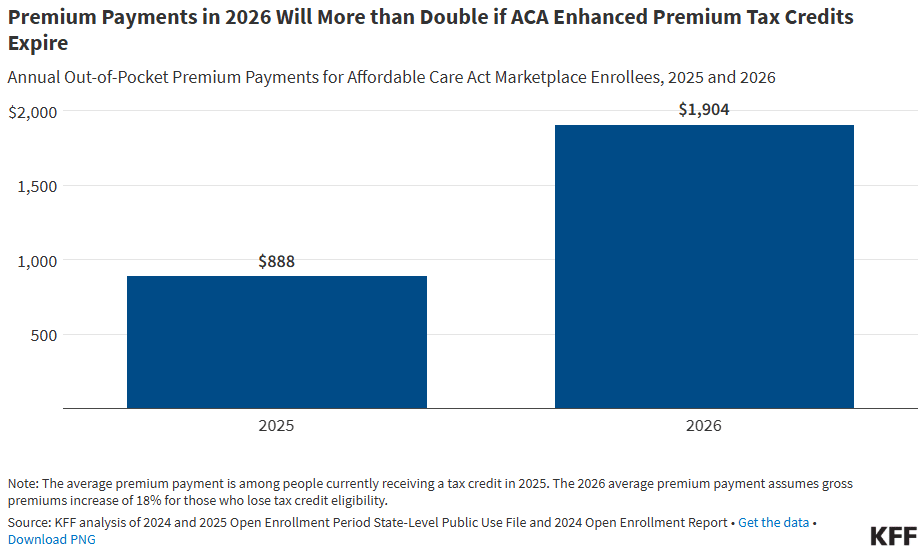
And, the study cited above was in 2022.Fast forward to today, and that same family of four’s finances would be stretched thin. Like really thin. On average, the monthly health insurance cost for a single adult is now $752, an increase of $129 without the subsidies. That’s an extra $1,554 PER YEAR and only includes one person. If your annual household income is $22,000-28,000, your annual premium payment goes up ~$1,200. Read that last sentence again - the annual income of $22,000-28,000 translates to $1,833-$2,333 a MONTH. You can barely pay rent, utilities, and buy food for that as a family. So, adding an additional $129 to keep your health insurance is brutal.
Along with the ACA premiums, there are tax credits associated. Those were set to expire at the end of 2025 (although some states have come in to lessen the blow). The double whammy of losing both the tax credit and higher premiums is shocking. Premium payments will more than double if the tax credits go away. For a family of four, health insurance is now largely out of reach.
In my day job, I study the intersection of poverty and children’s health. The number one reason that families get thrown into poverty is because of high healthcare prices. And, that’s if they even decide to go to the doctor. Many, many families have to make a decision between going to the doctor when they need it or wait because it’s too expensive (and they need to buy food). In the US, an estimated 75% of uninsured adults delay healthcare because of the cost. For many conditions, waiting means the condition gets worse and continues to do so until they finally have to go to the doctor (or more likely, the ER and accrue $$$ in medical bills).
These are called impoverishing or catastrophic expenditures. Another way to think about it is this - families are one or two catastrophic health events away from poverty. You go to the ER one time and incur lots of medical debt - which you can’t pay off - so you have high interest rates - that you can’t pay off. So, you pay the minimum while also trying to pay for food or housing. Do you see the cycle of poverty perpetuated and continued by just one ER visit (or urgent care or doctor’s visit)? Families that live on the brink of poverty or in poverty already are one visit away from impoverishment. That’s a catastrophic expenditure.
And, that’s what I spend all of my working hours trying to figure out how to solve. Sure, we could throw money here and there for families. But that would only be a band-aid to a gaping wound. I also totally get that the entire health system could be overhauled to make healthcare in the US more affordable (but that’s a whole other post).
But today, especially today, families need to be able to access healthcare when they need it, and not have to worry about whether they can put food on the table that night.
Affordable healthcare and health insurance are doable. And, that brings me to neighboring. Without the subsidies, 22 million Americans are at risk of losing insurance entirely or incurring medical debt. Already, 36% of US households have some form of medical debt, and 3 million owe more than $10,000. Each year, 67% of ALL people who file for bankruptcy do so because of medical bills. With all things in neighboring, the burden of medical debt is not equal. Our low-income, uninsured, and Black or Hispanic neighbors bear a disproportionate burden.
Medical debt is also one of the main drivers of housing instability - especially if you have a single-family home with children.
I guess what I’m trying to say is that affordable health insurance matters.
It not only matters to a person’s or a child’s health. It matters whether or not that family can buy food and stay in their home. It’s a compounding effect that is not equal and a downward spiral that is extremely hard to get out of.
Why focus on medical debt?Because it is usually one of the first on-ramps to poverty. And, it makes sense if you think about it. If your child or family member is really sick or hurt, you’re going to want to get them to care as quickly as possible. We will do what it takes to care for our children, especially if the situation is dire. So, that make-or-break moment turns into a ‘full break’ moment when the ER bill is too much and you don’t have insurance or a nest egg to cover it. How do you get out of that spiral when you’re still trying to buy food? It’s extremely hard and not as simple as pulling yourself up by your bootstraps. Especially when you haven’t been able to afford those anyways.
So, why medical debt? Because it’s the main driver of housing insecurity, a main driver (the main?) for poverty, a contributor to food insecurity, and a cycle that’s hard to get out of.
And, also.
It’s a keystone moment for intervention. Lowering people’s risk of debt (helping them afford healthcare and health insurance through subsidies like the ACA) not only helps them physically thrive but can keep them in their homes and able to feed their families.
That’s neighboring to me. And, sounds like the Good Samaritan story, doesn’t it? Remember when the good Samaritan helped bandage up the hurt man on the side of the road? AND THEN took him to a place to recover and told the innkeeper that he would pay for it all?!? I mean!! This story is layered with nuance for today. It’s not just about bandaging up people’s physical needs. To me, it’s also about making sure they aren’t bankrupt from medical expenses (including the recovery time).
To me, that’s why medical impoverishment and the ACA are ‘neighbor’ issues. (That’s why I wrote an entire book about health equity, loving our neighbors, and the Good Samaritan story. Here’s the Bookshop link (support your local bookshop!) or Amazon link.)
“And he paid for all of it.”
That sounds like government systems that are aligned more like the Good Samaritan story, doesn’t it. (And, fun fact, subsidies like the ACA or assistance programs like SNAP benefits are actually good for the whole economy too - but that’s for another post).
Keep neighboring, friends. You’re doing great work!
-Emily
Friendly Neighbor Epidemiologist is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
February 6, 2026
Talking about capitalism, structural violence, and ICE at the National Prayer Breakfast
Whoa. What a weird experience to be in a room with Trump, Hegseth, Kristi Noem, Paula White, Pam Bondi and others. I’m not sure how to start this - but, the National Prayer Breakfast was weird, FULL of Christian Nationalism, and everything-opposite-of-Jesus. Where Trump and Hegseth openly mocked people in the room, mocked Minneapolis’ deaths, mocked immigrants - and people stood on their feet for it. Hegseth said that peace comes through power and strength (alluding to violence) - because the Bible said that’s the way peace comes. Wait, what? Not my Bible. That’s when I walked out of the room. It was all expected - and still awful and shocking. Scary, maddening, ruthless, reckless, unconscionable. I was the only one that I could see that wasn’t standing up. Even when Trump came in and you’re supposed to stand up for a President - I refused to stand. And got looks and loud claps while a lady glared. It’s a small act of resistance and I’m sure there were others in the room who stayed seated (although I couldn’t see them). But, I refused to stand up for people blatantly mocking people who died or immigrants or…all while usurping the words of Jesus for power and privilege - in the name of ‘religion’? “Woe to those who make unjust laws and oppress the poor…” Trump said that he is bringing religion back to the US and called for a national day of prayer in May to do so. That religion is one of war, hate, and power, though. It is certainly not Jesus.
After the rambling-anti-Jesus talks that were more like a campaign speech, I gave my remarks in another room to a smaller group of people. Before I started, a man came up to me aggressively because he read the beginning of my book and asked, again aggressively, “How exactly do you propose policies that would combat racism?” Alright, then! I proceeded to tell him the answer, and he kept interrupting me, over and over again, louder with more aggression. I kept backing away from him, and he would just get closer. I finally told him to quit interrupting me, listen to my talk in a minute, and I walked away from him (you could tell he was not happy about that).
There is an aggression, a violence to Christian nationalism that was evident all throughout the event. You could hear it from the podium by Trump and Hegseth and feel it in the rooms. There was also a loud cry to increase too - increase the hateful rhetoric, increase ICE, increase the “scary and powerful guards”, increase power through force and “strength”. That’s not religion. That’s nationalism. In the coming days, it will be all the more important to combat that with the truth of who Jesus is and what Jesus modeled to us (particularly in the Good Samaritan story). The Good Samaritan story is one that is about as opposite to Christian nationalism as you could get and has themes pushing against power, privilege, capitalism, and ICE - which is exactly why I talked about it in my speech (see below).
If anything, this prayer breakfast made clear that neighboring will continue to be hard, increasingly so. We desperately need people who believe in the true words of Jesus (that never said peace is achieved through strength, for the record) to stand up (or sit down in rooms where everyone else is standing up for injustice). Speak up when you can and walk away when you need to.
But, we always neighbor. Always. Loudly. Diligently. Together.
I’ve included my remarks below. I only had 8 minutes, so I tried to squeeze in as much as I could. If you want the full version of these stories and stats, my book (here and here) goes into detail for all.
Here’s what I said:
When I was growing up, I wanted to be two things: Sandi Patty and a missionary. But I also loved science. Like, loved, it.
I thought the only way to combine all of that was medical school. Until I went on the Mercy Ships. And noticed I was asking questions about poverty and geography, systems and politics, rather than traditional medicine. So, I decided to get a PhD in epidemiology when my professor said the science of epidemiology is figuring out where the inequities are, which are almost always on the margins, and doing something about it. As a person of faith, it hit me that…
Epidemiology was the Science of the Good Samaritan story. It’s a science of quantifying the most at need and choosing not to walk by.
Most of us are familiar with this story, but if we look closer, it's a sneaky story on equity, neighboring, and justice. It’s a story of a man who asked Jesus a question to trap Jesus. “Who is my neighbor?” It was a non-question question of “What is good enough to be good enough?” But, Jesus did what Jesus does and answered with a story. He told a story of a man who was hurt on the side of the road. Two people of power and privilege of the day walked by that man before a Samaritan man stopped, bandaged him up, took him to a place to recover, and paid for all of it. Then Jesus turned to the man again and asked a question.
“Who was the neighbor?”
If you don’t look closely, the questions look the same, don’t they? Who is my neighbor versus who was the neighbor? But they are very different in rhetoric and action.
Do you see the difference in postures? Worldviews? One asked what is good enough to be good enough, while the other neighbored as a verb. Extravagantly.
At the center of both questions was a person in need on the side of the road who had been walked by twice by power and privilege.
There is an extravagance to neighboring that is more than just sponsoring a child or giving money to a food pantry, which are all good. Neighboring, though, is something more - it’s surrounding the man with everything he needs in the story - and more. So how do we live as neighbors in both heart and deed today in a world set up to do the opposite? Answering this question will require faith, and/also require recognizing the margins themselves – as individuals and systems.
I need to tell you about two places I work: Somaliland and Rwanda, which I just returned from last week. These are countries with some of the highest maternal mortality rates in the world, with women traveling hours by foot or wheelbarrow to the hospital. One of the main complications is pre-eclampsia. I had severe pre-eclampsia with my second child, with both of us being in the hospital for a while. But I had healthcare access close to my home, insurance, and a nest egg to cover costs.
In places like Somaliland, that is not the case. The risk of dying from pre-eclampsia for a women just like myself is 14 times higher there than in the US. But here’s the important part: It’s of no fault of her own. It’s the systems, structures, policies, or lack thereof around her. It’s a violence but not an individual one. A structural violence. When that is overlayed with systemic racism and unjust policies, with decades of under-funding aid and colonialism, of modern-day walking by of power and privilege, women and children will die – again, of no fault of their own. Being a neighbor means we see the individual women and babies, and also see those oppressive systems around them.
Many of you will remember the Ebola crisis that happened in West Africa in 2014. One of the leaders was Dr. Khan, who was very well known. In fact, he came to the US years before asking for help to build up his country’s health system in case something like Ebola happened– to no avail. So, when Ebola hit, it hit hard at his own hospital, where he treated several patients before getting sick and deteriorating quickly. Now, Ebola is not a deadly disease. It is only deadly without supportive care, and because of structural violence. At the facility, there was an experimental vaccine for Ebola, but there were only a few vials in the world. After lots of deliberation, it was decided to not give Dr. Khan the vaccine, and he would die a few days later without his family. In a neighboring country within the same timeframe, another physician and a nurse got sick with Ebola, both Americans with connections of money and power. Same story with quick deteriorations, and again a decision having to be made. They not only received the vaccine but would later be transferred to a state-of-the-art hospital in the US, and both walked out alive weeks later. Now, I want to be clear that if this were my family member, you better believe I’m moving heaven and earth to get them care. You would too. But, that’s not the point of the story. The point as neighbors is who gets to determine the value of a life of a person? Or a country or a community? Dr. Paul Farmer said ‘The idea that some lives matter less is the root of all that is wrong with the world.” Living as neighbors means valuing all lives, all countries, all people equally. And we have enough to go around.
You might remember a picture of rows and rows of funeral pyres from the second wave of COVID in India where cases would peak at over 400,000 cases per day and last for weeks. The unimaginable magnitude of the pandemic on the country took its toll on the healthcare system, where the country ran out of oxygen in the urban centers. In one ICU with 24 patients, 21 patients would die through the night. Because they ran out of oxygen. This is an issue of why the oxygen wasn’t there in the first place. Why healthcare systems don’t have what they need equitably? When high-income countries gobbled up 80% of the world’s stockpile of vaccines and oxygen during the pandemic, who gets to measure who gets what? Or, in one year after the dismantling of USAID, 500,000 children have died and 90% are in low-income countries like I work in. In Tanzania where I work, we saw mothers not able to get life-saving medicines for their children. That’s not neighboring and certainly not Jesus. That’s structural violence.
And those structural or systemic choices affecting countries because of power matter today for real individual lives. I guess another way to say all of this is, it matters where you were born. Maybe a better way to say it is, it matters what you were born into.
Which brings me to the US and children’s literacy.
Let me show you a map of redlined districts in Durham, North Carolina where I’m from. During the Great Depression, the federal government created the Homeowners Loan Corporation. Prior to giving out the loans, they sent representatives to neighborhoods to determine who would qualify for a loan. If you lived in a predominantly Black neighborhood, it was almost entirely deemed as hazardous, and adjacent neighborhoods were deemed declining. Of the 2.7 million loans given, just 50,000 went to Black families, half of which were under a military housing program. The impact of this unjust power, this structural violence, reverberates to today, with home values being over $200,000 less in redlined neighborhoods. Those neighborhoods continue to have increased food insecurity, lack of grocery stores or green spaces, and lack of health clinics. And the highest rates of childhood illiteracy. The point of the story is to remind us that the history of a place, including the historical wielding of unjust power, impacts the present. It’s not just about child literacy – it’s about everything else surrounding those children – or not. Thinking like the Good Samaritan means we do not shame the neighborhood or people in it for not having enough greenspace or a poor performing school or who desperately need SNAP benefits. Neighboring here means recognizing there’s a history to be told.
A structural violence to be accounted for.
With nearly 50 percent of the world’s wealth held by only 1 percent of the richest people and access to healthcare and books limited by geography, maybe we have our starting points wrong? Maybe these are our modern-day ‘walking bys’. Maybe being a neighbor today means we start with the poor first. We clothe, we feed, and also we dismantle oppressive systems, tear down systemic racism, and we remember Isaiah’s words of “Woe are you who make unjust laws, to those who issue oppressive decrees, to deprive the poor of their rights and withhold justice from the oppressed” and Micah’s call of justice, love, and mercy.
What about a trickle-up system rather than a trickle-down system that starts with the margins first – with children who need food and literacy and mothers who love them? My work as an epidemiologist shows that starting with the poor first actually benefits societies more than capitalism – but that’s for another talk. Maybe here today, we need to talk about tables of power and privilege that walk by like the two in the Good Samaritan story. And we flip them over to build a new equitable table.
I think neighboring does that to us. It interrupts us individually and collectively and asks us to a new table. That table of neighboring can be a healing table for our nation – but only if we have recentered on the margins Jesus centered on. Jesus centered on the little children and the immigrants. Not detain them. He stopped entire crowds and centered the medically impoverished women. Not shame them.
This is a merciful table, a neighboring table that looks like heaven when the lowest person is at the head and where the marginalized have been brought to the center. When all have enough to eat, to share, and to be satisfied with extra baskets. A table of color and equality and children being able to read. This is a table of not just enough, but abundance. Where we ask for our daily bread and also for it to be multiplied for others. Not just for individuals but when our power structures, policies, and politics don’t walk by either.
A table where we recognize the sacredness in the other and makes us take off our shoes because the ground there is holy. That’s what a neighboring looks like to me.
I hope that when we are asked, “Who was the neighbor?”, we have lived out our faith in the margins, both the people and the structures, and we can answer with a resounding “It was me.”
February 1, 2026
Home from Rwanda and headed to the White House
I’m back home from a few weeks in Rwanda with a heart full. And, some trepidation. I came home to a US ravaged by ICE, including the horrific killings. There’s a new policy after new policy from the administration that is dismantling safety nets for people, resulting in families going hungry or not getting healthcare they need. When I travel, I have a rule to not follow the news back home and just ‘be’ wherever I am. I did that, for the most part, in Rwanda. But the little boy being taken by ICE and then the killings by ICE agents changed that for me.
January 23, 2026
Neighbor Thursday: Hello from Rwanda!

Hi neighbors!
I’m writing to you from the gorgeous country of Rwanda. They call this country the land of a thousand hills, and I can believe it! It’s hill after hill after hill - dotted with different shades of green that look like a patchwork quilt. It’s stunning. I keep saying it looks like a calendar picture or something you’d see on a screenshot. It takes your breath away.

I’m here at the University of Global Health Equity (UGHE) in Butaro - which is north Rwanda, almost to Uganda and close to the Democratic Republic of Congo. You can see Mount Muhabura, an extinct volcano on the border between Rwanda and Uganda when the sun is out. Do you see it in the picture below? Told ya - stunning!

In 2014, UGHE was founded by Partners in Health and Dr. Paul Farmer. If you’ve read my book, you know that it is, in part, dedicated to Paul, and there’s a whole chapter dedicated to him. So, to be here, at his place of vision for health equity is hard to put into words. I’m here with my favorite collabo-colleague-friend, Dr. Henry Rice (also in the book lots of times, including in the dedication!). We are teaching a group of students getting their Masters in global health delivery, specifically in the global surgery track. It has been, by far, my favorite part. At the end of the week, UGHE will graduate their first cohort of medical students on Sunday! And, it will be such a joyous occasion with families coming in.
This post really isn’t about any data or statistics. It’s more about what I’ve been thinking about this week - what it looks like to be a neighbor here and how that changes us. It’s in the ‘doing’ part of neighboring that continues to surprise me - not in the sense that the ‘doing’ is transactional in that we love our neighbors and then we get something out of it. That’s paternalism or colonialism or both, not neighboring. Neighboring is giving, loving, serving. And, that’s it. Yet, it’s in the ‘neighboring’ as a verb (the ‘doing’) that changes us from the inside. It’s not transactional. It’s transformative. Again, we don’t ‘neighbor’ to get anything out of it. We simply neighbor. And then are changed. At least for me, that has been the case. Not only are we changed, but we are strengthened, encouraged, bolstered, and challenged.
For me, it has felt like you’re caught up in a richness or extravagance or abundance of the world through neighboring. And, that changes you to be a better, more equitable neighbor. (For those of you in the Christian faith tradition, I keep thinking of Ephesians 2:4 and Lamentations 3 about a great love, rich mercy, steadfast faithfulness…) I also wonder if that richness or over-abundance of life that comes through neighboring is only found by neighboring. At least for me, that’s the only way I’ve found it. As human beings, I wonder if that’s the case for all of us.
So, I want this post to be a bit more of an encouragement to you all. Being a neighbor in ways that take courage has changed me more than I’ll probably ever be able to put into words. (Especially since I don’t consider myself a courageous or loud person - it doesn’t come naturally to me.) It’s in the ‘doing’ of neighboring that I have found an over-extravagance of life that feels like I can stand up to my full height, breathe deep, look up, and smile. I hope that for you today. That in the daily ‘doing’ of neighboring in whatever way that looks for you (changing diapers, saying hello to a friend, caring for the sick, donating to a food pantry), you would be caught up in that richness yourself. And, it sustains, bolsters, strengthens, and encourages you. There’s joy for this neighboring journey, friends! It just might catch you by surprise in the ‘doing’.
In solidarity (the word Paul taught me and the title of the book chapter I told you about),
Emily


